Answer: Yes, Ok so im going to help you out! Answer:
Diabetes can lead to eye problems, some of which can cause blindness if not treated: ... Having diabetes puts you at higher risk for gum disease. ... eat right, exercise, lose weight, avoid smoking, and get high blood pressure and high cholesterol treated.
Explanation:Being overweight (BMI of 25-29.9), or affected by obesity (BMI of 30-39.9) or severe obesity (BMI of 40 or greater), greatly increases your risk of developing type 2 diabetes. The more excess weight you have, the more resistant your muscle and tissue cells become to your own insulin hormone.
Hope this helped!
The type of psychotropic drugs are not found here but they can be classified into antidepressants, anti-psychotics, anti-anxiety, stimulants, and stabilizers.
<h3>What are psychotropic drugs?</h3>
Psychotropic drugs are specific medications (drugs) capable of affecting human behavior, emotions, and perceptions.
The type of psychotropic drugs used in a given treatment is variable according to the mental (cognitive) disorder.
In conclusion, the type of psychotropic drugs are not found here but they can be classified into antidepressants, antipsychotics, anti-anxiety, stimulants, and stabilizers.
Learn more about psychotropic drugs here:
brainly.com/question/11129212
#SPJ1
Answer:
Misdiagnosis
Explanation:
If you do not have a complete medical file, you can misdiagnose the patient.
Answer:
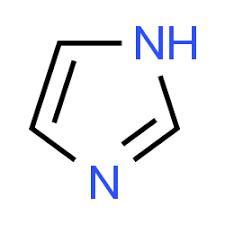
See explanation and image attached
Explanation:
The structure of imidazole is attached to this answer. The compound is colourless. The solid can be to dissolved in water leading an alkaline solution. Owing to the fact that imidazole possesses heteroatoms in an aromatic heterocycle it is classified as a diazole. The nitrogen atoms in imidazole are not adjacent to each other.
From the structure shown, we can see that the lone pair of the sp2 hybridized nitrogen atom is available because it is not part of the aromatic system of the heterocycle. This nitrogen is much more basic than the nitrogen atom attached to hydrogen whose lone pair becomes part of the aromatic sextet hence it unavailable for protonation and less basic.
The assessment finding that is important is Continuous trickling of blood.
<h3>What is hemorrhage?</h3>
Hemorrhage is defined as the release of blood from a damaged blood vessels into a surrounding tissue.
A postpartum client is an individual that has just been delivered of a baby through the normal birth canal.
When there is laceration of the cervix the nurse should find out if there is still trickling of blood as this is a sign that there is still ongoing internal hemorrhage.
Learn more about hemorrhage here:
brainly.com/question/18039247
#SPJ1